Professor of Rhinology & Skull Base Surgery, Ain Shams University, Cairo, Egypt
Department of Oto-Rhino-Laryngology, Faculty of Medicine, Ain Shams University, Cairo, Egypt.
11- Endoscopic Skull Rhino-Base Repair
The skull base is crowded with many vital structures such as the great vessels, cranial nerves and organs of special senses. The ventral (anterior) skull base is related to the orbit, the nose and the first six cranial nerves. Due to its complex nature, skull base lesions are usually difficult to be early diagnosed and properly assessed.
Surgery is the primary treatment modality for the majority of such lesions. To reach deep areas, normal structures are either extirpated needing subsequent reconstruction or mobilized needing subsequent reposition and fixation.
Injury to the cranial base with failure either to recognize the insult or to repair it may lead to cerebrospinal fluid (CSF) leaks and/or meningo-encephalocele formation. Spontaneous CSF leaks occur in absence of a history of accidental or operative trauma. For both traumatic and spontaneous CSF leak groups, the CSF pressure might be normal (normotensive leaks) or high (hypertensive leaks). In hypertensive leaks subarachnoid-peritoneal or subarachnoid-venous shunts are commonly needed following the leak repair.
Recent advances in imaging, visually aided techniques and navigation systems facilitate management of such skull base lesions. Diagnosis of CSF leak is confirmed with detection of Beta-2 transferrin protein in the fluid. Localization of the site of leak is reached with imaging, endoscopy and sometimes intrathecal fluorescein.
Imaging:
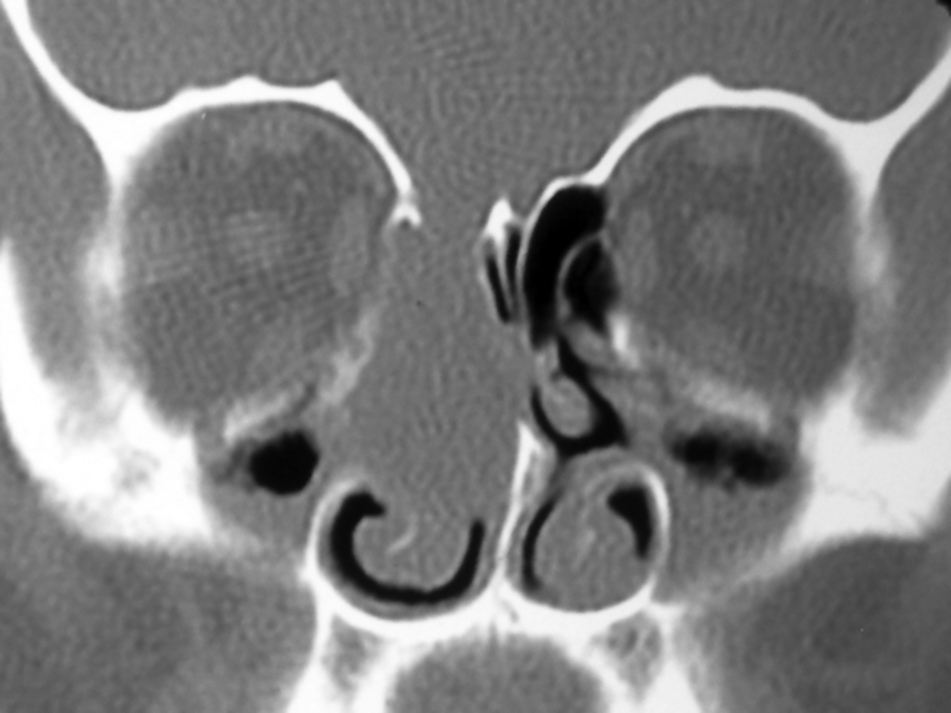
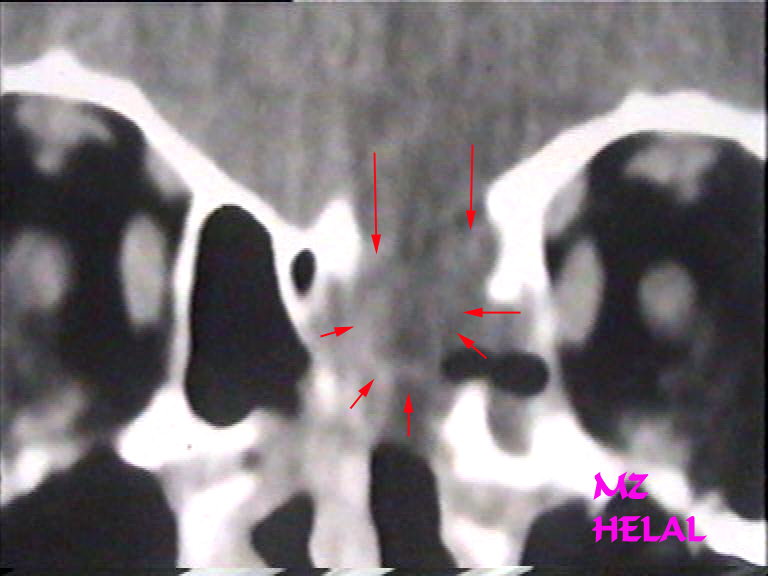
High resolution multislice CT fine-cuts (1.5 mm) may visualize bone defects and meningoceles (when small called micromeningocele). With Intrathecal dye, the smallest defects can be detect provided the leak is active.
MRI T2 cuts may detect CSF density fluid in one sinus or air cell in absence of concomitant sinus disease.
Endoscopes:
Endoscopes position the surgeon nearest to his target. By their angled vision, endoscopes are the only tools that directly visualize the skull base. Angled endoscopes (30, 45 & 70 degrees) offer end-on visualization of the anterior cranial fossa floor. Moreover, endoscopes visualize hidden recesses minimizing radical extirpation of normal structures and the later need for reconstruction. In addition, endoscopes minimize mobilization of normal structures and therefore the need for subsequent reposition and fixation.
Microscopes offer magnified, binocular vision perceiving the third dimension. However, their straight vision give tangential view for the skull base. Therefore microscopic surgery is suitable only for few repairs involving posterior-situated midline structures such as median portion of sphenoid and the sella turcica that can be seen efficiently with the straight microscopic view.
Techniques of CSF Leak Repair:
Steps of repair of meningo-encephaloceles and CSF leaks are:
1- Localization of the defect.
2- Preparation of the site of the defect for grafting (5 mm bone raw surface around the defect).
3- Multi-layer grafting: fat, fascia, mucosal graft, cartilage and/or bones (for defect >1 cm).
4- Glue: human fibrin glue, surgicel and rarely Histoacryl.
Skull Base Repair Techniques: Movie A
Skull Base Repair Techniques: Movie B
Video Demos Of Interesting Cases:
1-
Movie 1: 64 y.o. male
patient with left spontaneous CSF rhinorrhea for few months that failed to stop with
conservative management.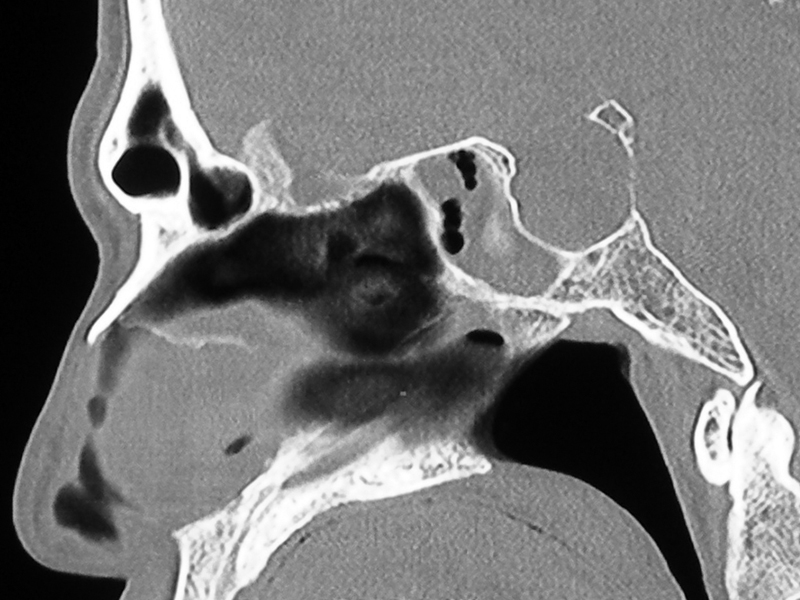
Skull Base Repair Patient 1 Movie
2- Movie 2: 42 y.o. female with recurrent bouts of severe headache with visual blurring for years, left spontaneous CSF rhinorrhea for three months and failed conservative management.

Skull Base Repair Patient 2 Movie
3- Movie 3: 38 y.o. female patient with recurrent left watery rhinorrhea for 2 years proved to be spontaneous CSF leaks which failed to be controlled conservatively.

Skull Base Repair Patient 3 Movie
4- Movie 4: 52 y.o. female with right-sided CSF rhinorrhea for 3 months following nasal surgery elsewhere.
Skull Base Repair Patient 4 Movie
5- Movie 5: 31 y.o. male presented in 1998 with left CSF rhinorrhea for 4 months following nasal surgery elsewhere.
Skull Base Repair Patient 5 Movie
6- Movie 6: 43 y.o. male with history of repeated head trauma, presented in December 2001 with right CSF rhinorrhea.
Skull Base Repair Patient 6 Movie